

Very often we hear about inflammation or injury of tendons, but what is the difference between these two conditions?
Tendinitis is the term for an inflammatory process in the tendons, characterized by severe pain and often swelling and redness of the area affected by inflammation.
Tendinosis, on the other hand, is the clinical name that indicates the presence of a process which damages the anatomy of the tendon, and can lead to the rupture of the tendon. Tendon injuries are very common in sports because the tendon structure is more rigid in athletes to allow for high sports performance, but as a consequence can lead to damaging processes.
Both tendinitis and tendinosis share a common symptomatology that is usually called tendinopathy, indicating a complex pathological condition, characterized by pain and a reduced function and tolerance to movement. Moreover, some studies have reported that this condition can reduce the quality of life of those affected, as well as impact daily activities.
Anatomical notes: a tendon
A tendon is a bundle of connective tissue that binds muscles to bones.
Tendons are composed mainly of type I collagen protein fibres as well as various substances, such as proteoglycans, glycosaminoglycans, glycoproteins and other collagen proteins (type III, IV, XII).
This particular composition guarantees both strength and elasticity, in fact the tendons are designed to withstand the forces generated by the muscle to allow movement.
Types of tendinopathies
The cause of tendinopathies is generally multifactorial and complex, although the pathological process is due to an overload and this leads to a structural change of collagen fibers.
Tendinopathy occurs more frequently in middle-aged or elderly people, as tendon structures appear weaker and are therefore more susceptible to injury and inflammation.
On the other hand, the majority of tendinopathies in young subjects are due to intense and repetitive physical activities, which subject the tendon to excessive overload.
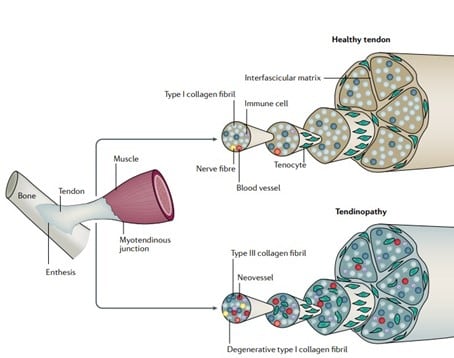
Figure 1 - Source: Neal L. Millar. Tendinopathy. Nat Rev Dis Primers. 2021 Jan 7;7(1):1
Figure 1 illustrates the difference between a healthy tendon (top) and a tendon suffering from tendinopathy (bottom). In the first case we mainly appreciate a well-organized network, composed of collagen fibers type I, while in the second case, the fibres are degenerated, causing less elasticity and strength to the tendon itself.
Tendinopathies are commonly found in the upper and lower limbs, as illustrated in Figure 2, below.
• Tendinopathy of the shoulder
• Tendinopathy of the heel
• Tendinopathy of the elbow
• Tendinopathy of the knee
• Tendinopathy gluteal

Figure 2 - Source: Neal L. Millar. Tendinopathy. Nat Rev Dis Primers. 2021 Jan 7;7(1):1.
The risk factors that lead to a case of tendinopathy are different and may depend on the type of sport practiced, types of work, the presence of systemic diseases, being overweight and even a certain genetic predisposition.
In addition, it has been shown that the use of certain antibiotics, such as fluoroquinolones, or the abuse of corticosteroid drugs can increase the risk of tendinopathy and tendon rupture.
The management of tendinopathies
There are different approaches to dealing with tendinopathies, but they all aim to reduce symptoms – especially pain – promote recovery and increase function.
Treatment regimens can be divided into two types: passive regimens which include pharmacological treatments, injective therapies, ultrasound therapy and laser therapy; and active regimens, which consist mainly of physiotherapy, patient rehabilitation and load management.
Therapy depends on the stage and progression of the disease:
- Acute tendinopathy The recommended treatment in this case provides total rest from physical activity; the use of anti-inflammatory drugs (NSAIDs) is useful only in cases where the inflammatory process is very marked. Instrumental therapy, such as laser therapy or diathermy, is useful to restore the strength of the muscles and tendons involved.
- Chronic tendinopathy The resolution in this case focuses mainly on the gradual recovery of mobility through eccentric exercises, which consists in stretching the muscle tissue to the maximum and consequently lengthening the tendons connected to it.
Cetylated fatty acids (CFAs)
An important aid for the management of the painful symptomatology of tendinopathies comes from Cetylated Fatty Acids (CFAs) patented by Pharmanutra S.p.A. in Cetilar® products.
CFAs are a mix of fatty acids of plant origin that have proven to be effective in reducing muscle-joint and tendon pain. The product line Cetilar® for topical use consists of:
- Cream
- Patch
- Tape
The mechanism of action of CFAs is to promote joint lubrication and therefore to improve mechanically the movement of the joint. In addition, it has been shown that the beneficial effect produced by CFAs, applied by therapeutic massage in subjects with osteoarthritis pain syndrome, could be mediated by the mechanical modification of the synovial membrane, thereby reducing painful symptoms.
A recent study involved subjects with shoulder tendinopathy, with the aim of evaluating the efficacy and tolerability of Cetilar® Patch.1 All subjects applied the Cetilar® Patch for eight hours a day for 10 consecutive days, without recourse to any other type of instrumental or pharmacological treatment. Through a specific evaluation scale, the pain and functionality of the shoulder were evaluated during the first visit, after 10 days from the first visit and in the subsequent follow-up after 35 days.
The results showed how the application of the Cetilar® Patch for 10 consecutive days was useful in reducing pain and increasing joint function in people with shoulder tendinopathy. In addition, it is particularly interesting to note the maintenance of the beneficial effect obtained, even in the follow-up, without applying the Patch anymore.
In conclusion, Cetilar® products, are useful in improving joint mobility and in reducing painful symptoms in the joints, musculoskeletal and tendon, even in cases of sports injuries, allowing subjects to quickly return to normal daily activities.

References
1. Riel, H., Lindstrom, C. F., Rathleff, M. S., Jensen, M. B. & Olesen, J. L. Prevalence and incidence of lower limb tendinopathies in a general Danish practice: a register-based study. BMC Musculoskelet. Disorder. 20, 239 (2019).
Additional references
Hopkins, C. et al. Critical review of the socio-economic impact of tendinopathy. Asia Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 4, 9-20 (2016).
O'Brien, M. Tendon structure and metabolism. Scand. J. Med. Sci. Sports 7, 55-61 (1997).
Maeda, E., Noguchi, H., Tohyama, H., Yasuda, K. & Hayashi, K. The tensile properties of collagen fascicles collected from regenerated tissues and residues in the patellar tendon after removal of the central third. Biomed. Mater. Eng. 17, 77-85 (2007)
Andres, B. M. & Murrell, G. A. Treatment of tendinopathy: what works, what does not work, and what is on the horizon. Clin. Orthop. Relat. Res. 466, 1539-1554 (2008).
Neal L. Millar. Tendinopathy. Nat Rev Dis Primers. 2021 Jan 7;7(1):1.


